|
Higher toll cited from hospital errors
Wider definition used in new tally
CIDPUSA Foundation Helping Humans Welcome to the Back Pain section Go to back pain page
If you have been told you need surgery we can help you without surgery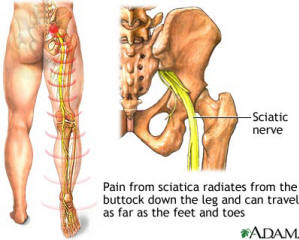
CIDPUSA Foundation Helping Humans Welcome to the Back Pain section Go to back pain page
If you have been told you need surgery we can help you without surgery Low back pain is one of the main reasons for a visit to a general practitioner. More than 95% of patients who have low back pain have a benign musculoskeletal pain syndrome; the pain is a manifestation of a more serious pathology in only 5%. Central disc prolapse causing cauda equina syndrome is only present in 2% of all cases of a herniated lumbar disc and in only 0.04% of all patients with low back pain. Herniation of an intervertebral disc is generally the result of degeneration of the disc. The inner nucleus herniates through the ruptured outside (annulus fibrosus) of the disc. The herniated tissue causes compression of dorsal roots in the spinal canal, which can result in pain, changed reflexes, and sensory and motor loss. The level of the herniation relates to the symptoms (table). In most cases lumbar herniations are at the level of L4-L5 or L5-S1. Herniation of the intervertebral disc mainly affects men aged 40-50. The rare diagnosis of cauda equina syndrome secondary to central disc prolapse is made on suspicion. Most patients complain of unilateral or bilateral leg pain and numbness in the perineum or leg or both.The most sensitive (0.90) and specific (0.95) finding is urinary retention or, later, even incontinence.Saddle anaesthesia and decreased sphincter tone on rectal examination, with sensitivities of 0.75 and 0.6-0.8, make the diagnosis even more plausible.Lasčgue’s straight leg test, which will cause pain by elongating the nerve root by passive flexion of the hip in a supine patient, is not very sensitive in this case. Onset can be gradual, as in this man, or sudden with acute trauma related sciatic pain and problems with vesicular control.Unlike most other back problems it may even be painless. The man had a partial laminotomy, and discectomy at the level of L4-L5 was successfully performed six hours after initial admission. He was discharged after four days, and apart from minimal sensory loss of his left foot he had no complaints at three months’ follow up. Competing interests: None declared. Provenance and peer review: Not commissioned; externally peer reviewed. Disc herniationLower back pain and bladder dysfunction
Discussion
Nerve Root Pain Sensory deficit Motor deficit Reflex deficit L2 Anterior medial thigh Upper thigh Slight quadriceps weakness; hip flexion; thigh adduction Slightly diminished suprapatellar L3 Anterior lateral thigh Lower thigh Quadriceps weakness; knee extension; thigh adduction Patellar or suprapatellar L4 Posterolateral thigh, anterior tibia Medial leg Knee and foot extension Patellar L5 Dorsum of foot Dorsum of foot Dorsiflexion of foot and toes Hamstrings S1-2 Lateral foot Lateral foot Plantar flexion of foot and toes Achilles S3-5 Perineum Saddle Sphincters Bulbocavernosus; anal
continued on next page
Lumbosacral Radiculopathy
Myofacial pain
Neck pain tips
Polyneuropathy and pain