Managing Myofascial Pain Syndrome
Dr Imran KhanRead the cause of myofacial pain
In Brief:Among the leading reasons for visits to physicians the cause is Myofacial pain, and about one third of these patients meet diagnostic criteria for myofascial pain syndrome (MPS). Although MPS was identified more than a century ago, debate over its existence as a separate clinical entity continues. Physicians who learn to identify characteristic symptoms can differentiate MPS from fibromyalgia and provide effective treatment. Key to treatment is identification of trigger points that when stimulated produce patterns of pain throughout a limb or region. Treatment modalities for MPS include trigger point injection, shiatsu, and the spray and stretch technique. Prognosis for MPS is better than that for fibromyalgia, and treatment usually follows an individualized regimen.
The musculoskeletal system comprises more than 400 individual muscles and is the largest organ system by weight in the human body. A recent study identified musculoskeletal complaints as one of the leading causes for patients to visit a primary care provider. As many as one third of these patients had symptoms that met the diagnostic criteria for myofascial pain syndrome (MPS).
Describing and Distinguishing the Pathology Simons et
Myofacial regional pain or MPS as a condition in which the patient has "hyperirritable spots" or "trigger points" within taut bands of skeletal muscle or fascia that are painful on compression and can give rise to characteristic referred pain, tenderness, and autonomic nervous system symptoms. Pain from MPS can be described as deep and achy, and it is occasionally accompanied by a sensation of burning or stinging. Patients may also report restricted range of motion in the area affected. MPS is limited to one area or quadrant of the body.
Treatment
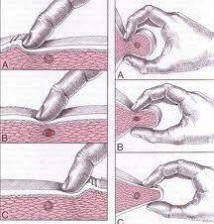
Treatment is simple Myofacial regional pain, find out where the trigger point is , if you simple run your finger over the painful muscle you may go over a speed bump. That is the trigger point and either massage it or strectch it or both. Hot and cold application also work. The pain is accompanied by cracking sounds , these sounds do not come from bones but tight muscle fibers. Vitamin D deficency is a big cause. See our other links on this painful condition.